"The psychology of thinking discretely"
« previous post | next post »
Andrew Gelman, "The psychology of thinking discretely", 10/20/2022:
Sander Greenland calls it “dichotomania,” I call it discrete thinking, and linguist Mark Liberman calls it “grouping-think” (link from Olaf Zimmermann).
All joking aside, this seems like an interesting question in cognitive psychology: Why do people slip so easily into binary thinking, even when summarizing data that don’t show any clustering at all:
It’s a puzzle. I mean, sure, we can come up with explanations such as the idea that continuous thinking requires a greater cognitive load, but it’s not just that, right? Even when people have all the time in the world, they’ll often inappropriately dichotomize. I guess it’s related to essentialism (what isn’t, right?), but that just pushes the question one step backward.
As Liberman puts it, the key fallacies are:
1. Thinking of distributions as points;
2. Inventing convenient but unreal taxonomic categories;
3. Forming stereotypes, especially via confirmation bias.
The comments on Andrew's post are interesting, though no one mentions the role of insurance companies and others to whom ICD-10 is the beau idéal :-)…
For more of my thoughts on the matter, such as they are, see the slides for a talk I gave last summer under the title "Generic Plurals Considered Harmful".
mg said,
October 20, 2022 @ 2:42 pm
Thank you for sharing your informative (albeit discouraging) talk. I used to do psychiatry research, so I especially appreciated "phenotypically diverse is the Greek translation of 'we have no fucking clue'".
Cervantes said,
October 20, 2022 @ 2:46 pm
Don't get me started on the DSM. With 5 of 8 criteria — all of which are matters of degree and the diagnostician's subjective judgment — you have Histrionic Personality Disorder. With only 4, you don't. It's all like that.
John Swindle said,
October 21, 2022 @ 1:42 am
I can't believe I'm defending DSM.
Psychiatrists and psychologists see people who believe themselves or are believed by others to have mental problems or disorders. They provide whatever relief they can and hope to be paid, if not by the patient then by someone else, so they can support themselves and their healing practice. But the payers want to know how many patients and what kinds of problems they've treated. Enter DSM. It serves a pragmatic purpose, for all its lack of explanatory power.
[(myl) I'm not an expert in the history of medicine, but I have the impression that medical theory at least since the Greeks has been based on assigning patients and their problems to "natural kinds". The categories and diagnostic criteria have frequently changed. Sometimes the idea works from a scientific point of view (e.g. "smallpox" or "gout"), and sometimes it doesn't (e.g. "hysteria" and "dementia praecox", and maybe also "autism", "schizophrenia", etc.). Modern medical and insurance bureaucracy strongly reinforces the need for these conceptual boxes. And there are perhaps benefits in terms of disciplinary training and patient community formation, even when the categories are "phenotypically diverse" and change boundaries (and even names) from era (or one edition of the DSM) to the next.]
John Swindle said,
October 21, 2022 @ 1:53 am
Of course that pragmatic utility depends upon there being some replicability between providers and that replicability not being better explained by racism or sexism or other ingrained prejudices, otherwise we are indeed back at the place Professor Liberman described.
Cervantes said,
October 21, 2022 @ 7:50 am
Actually no, the idea of diseases as discreet entities is entirely modern, dating from the late 19th Century. Until then, the prevailing theory was that illness was an imbalance among the 'humors,' i.e.black bile, yellow bile, phlegm and blood, and that treatment consisted of trying to restore the balance. This is actually like the Alternative Model of Personality Disorders the DSM is testing out because they know the current system is bullshit. Yes, it's used to justify billing but that's completely nonsensical.
Anyway, ,the reliability of DSM diagnostic categories is in fact very poor. People will get different diagnoses from different shrinks and their diagnoses routinely change over time.
Mark P said,
October 21, 2022 @ 8:34 am
@Cervantes — And yet people do have conditions that might benefit from some kind of treatment. The big problem is that the conditions are expressed as behavior, feelings or other symptoms that as yet can’t be determined by tests like we do for other health issues, like testing blood for thyroid markers. If we assume that there are different conditions that benefit from different treatments, then they have to be identified in some way. Of course, my own experience, through my wife’s treatments, indicates that in at least some cases, we are not doing a great job so far.
Terry K. said,
October 21, 2022 @ 9:15 am
Cervantes' initial comment on the DSM as it relates to the initial post, that it's too binary, makes a lot of sense to me. And interconnected with that, that differences that aren't considered disorders aren't classified at all, despite it being a diagnostic and statistical manual. The diversity in autism, the idea that it's a "spectrum" is recognized. Yet that there is a whole spectrum between autistic and neurotypical, people with autism traits that don't qualify as having a disorder, is not, for one example. Definitions of various neurodisversities that aren't disordered would be quite useful for statistical purposes, it seems to me.
Mike Grubb said,
October 21, 2022 @ 9:29 am
So what I hear you saying is that there are "natural natural kinds" and "non-natural natural kinds"…
Jerry Packard said,
October 21, 2022 @ 9:51 am
‘Phenotypically diverse’ rather means a range across the genotype. That genotype is bound to contain the seeds of ‘pathological’ phenotypes. It’s like Mark says: we need concepts and tools for dealing with continuous multi-variate distributions, the simplest of which is the dichotomous approach.
Rodger C said,
October 21, 2022 @ 10:03 am
phenotypically diverse is the Greek translation of 'we have no fucking clue'
I thought that was "idiopathic."
Jerry Packard said,
October 21, 2022 @ 10:43 am
Right you are.
Thomas Shaw said,
October 21, 2022 @ 3:20 pm
I enjoyed reading through these slides, and got a good laugh from the GPT-3 conversation. I passed it on to a friend, who responded with a paper on the subject. Maybe it will be of interest to some of you:
https://www.pnas.org/doi/full/10.1073/pnas.1817706116
Julian said,
October 22, 2022 @ 2:08 am
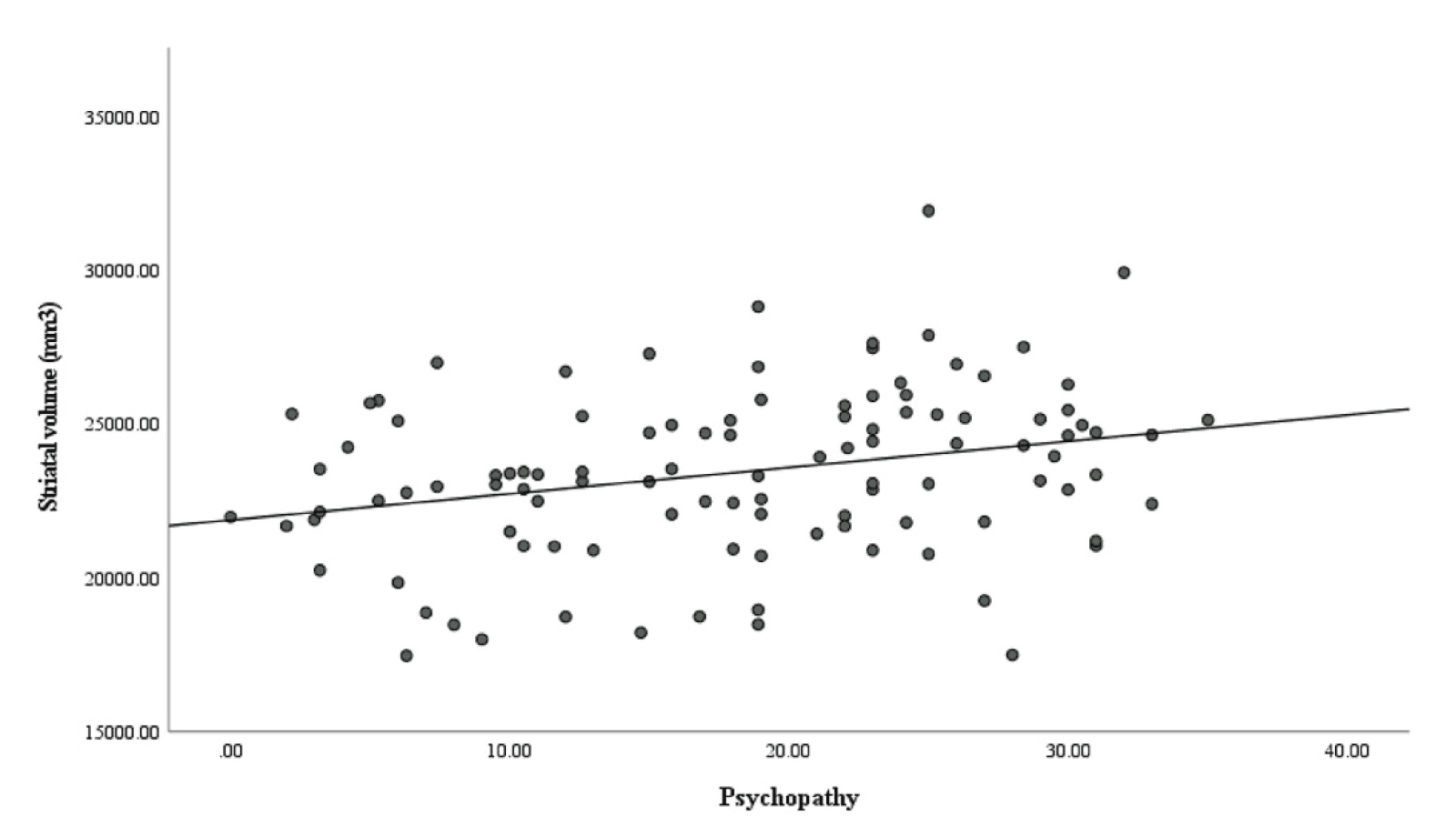
So having a big striatum causes psychopathy?
Now I'm worried!
Is there a Blackmores supplement I can get to shrink my striatum?
PS I'd love to know what the horizontal axis of the scatterplot means
Jerry Packard said,
October 22, 2022 @ 3:35 pm
We may not want to shrink our corpora striata. What happens if we take corpus striatum enlargement pills? No doubt the horizontal axis contains oodles of arbitrariness (= random error).